

The AI QA Signal Is Not Clinical Review
A consequential boundary between what gets human judgement and what doesn't.

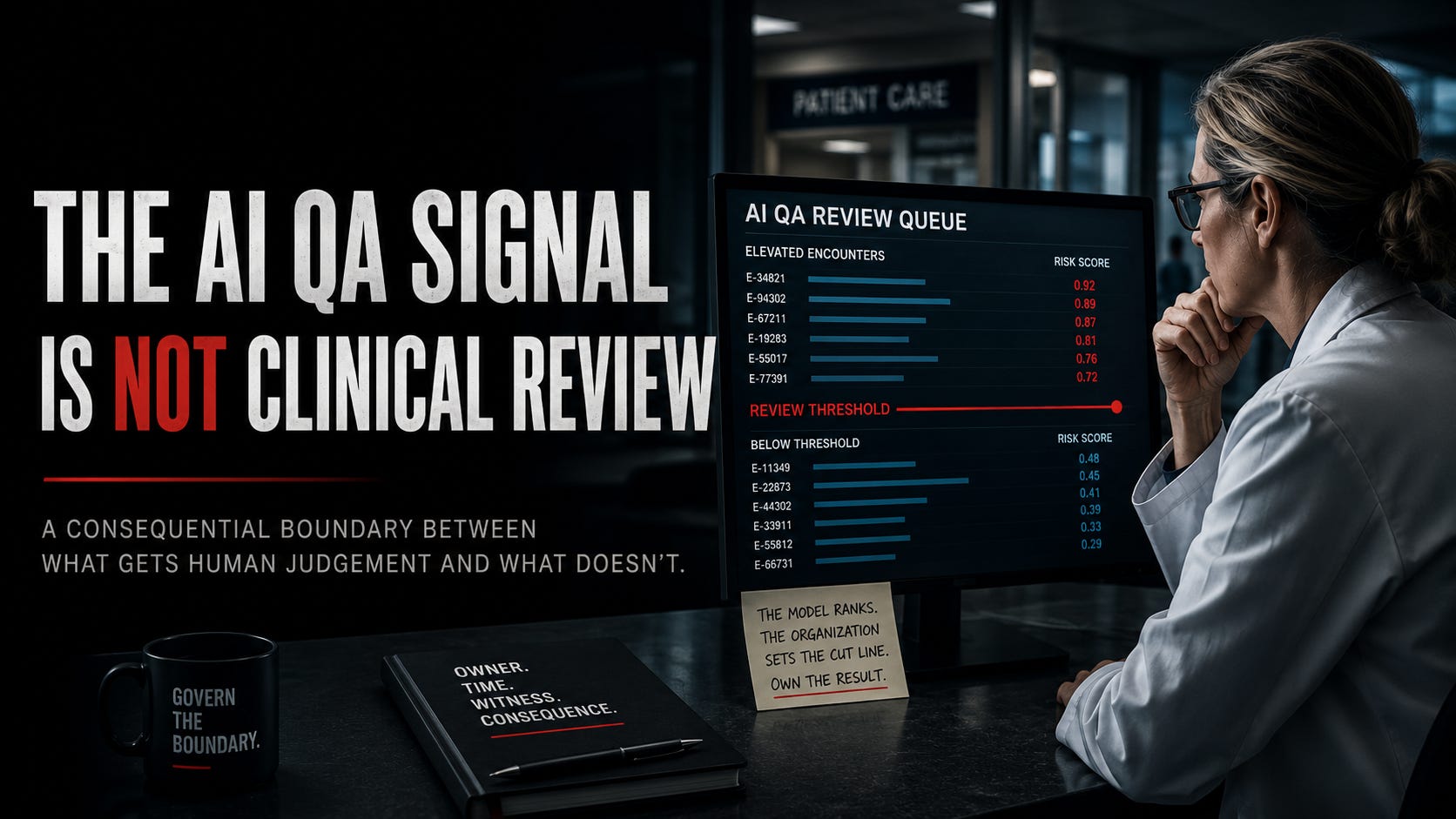
A quality reviewer opens the queue and sees the encounters the system believes deserve attention. Some are obvious. A concerning phrase in the note. A treatment decision that does not match the documented condition. A follow-up that never happened. The reviewer opens the chart, reads the record, applies clinical judgement, and decides what happens next.
From the outside, this looks governed. The AI found the signal. A human reviewed the case. The human made the call.
A consequential decision has already happened before the reviewer opens the first chart. The system decided which encounters reached the queue.
The Queue Is Already a Decision
AI-assisted quality assurance can solve a real problem. Clinical organizations produce more encounters than human reviewers can examine in depth. Manual review is narrow and expensive. What it examines is usually set by a complaint, a reporting obligation, or a risk the organization already knows how to recognize. A system that scans a larger population and helps experienced reviewers focus their time may improve coverage.
When an AI system ranks, filters, or elevates encounters in a way that determines what enters the review queue, it is allocating clinical attention. The reviewer still makes every formal judgement, but the system has already shaped the field in which that judgement will operate.
A queue is not a neutral list. It is the result of model behavior, prompt design, available data, and documentation quality. Mostly it is the result of a threshold, and of a decision about what kinds of risk matter enough to surface. It also reflects a less technical constraint that organizations are reluctant to name plainly. Reviewer capacity.
There are only so many nurses, physicians, and quality specialists available to read charts. The queue has to end somewhere. Someone decides how many cases the team can absorb, then the threshold is tuned until the visible work fits the human attention the organization is willing or able to fund.
Notice who did that. The model ranks. The organization sets the cut line. Those are two different acts with two different owners, and only one of them is a technical decision. A model does not know how many reviewers you hired. It cannot decide how much risk you can afford to see. A human decides that, and then the number comes back with the model’s name on it.
At that point, a staffing limit has been translated into an apparent judgement about clinical risk. The organization believes it is reviewing the riskiest encounters. It is reviewing the amount of risk it has capacity to see.
What the Queue Makes Visible
Most evaluations begin with the cases the system flagged. Reviewers ask whether the alert was useful, whether the concern was real, and whether the model elevated something worth examining. Those questions matter, but they only measure the population the system has already selected.
Flagged cases can be counted. They can be audited. They can be turned into evidence that the program works. A reviewer confirms the concern, an intervention follows, and the case becomes a success story. The program produces a receipt.
Missed cases produce no review receipt. Unless something else brings them back into view, the quality system records only silence.
A clinically important encounter can remain below the threshold because the documentation was incomplete, the language was ambiguous, the model did not recognize the pattern, or the risk appeared in a form the system was not built to weigh. It can remain hidden because the threshold was raised to keep the queue within staffing limits. None of those conditions mean the encounter was safe. They mean the system did not elevate it.
“Not flagged” then becomes “nothing to review.” After enough repetition, “nothing to review” becomes “low risk.” The queue begins to look like the territory instead of one instrument for looking at it.
A clean queue can conceal a dirty boundary.
The organization sees the cases the system surfaced. It has far less visibility into the cases the organization stopped expecting the queue to contain.
Human Review Starts Too Late
The phrase “human in the loop” does a great deal of reassuring work in healthcare AI. It implies that responsibility remains intact because a clinician is still present somewhere near the end of the workflow.
That framing is too shallow when the AI system controls practical access to review. The model scans the available population. The human sees the selected queue. By the time the reviewer begins, the system has already divided the encounter population into what receives scarce attention and what does not.
Human review does not correct a case that never arrives.
A careful, qualified clinician cannot challenge an omission they cannot see. They cannot reconstruct a pattern that was filtered out before the work reached them. The limitation is built into the path, not into the reviewer.
In any incident system, a queue is policy. What never pages is easily mistaken for what never mattered. Clinical quality assurance is not exempt from that logic merely because the queue contains charts instead of alerts.
The AI system does not need to replace clinical review to influence its outcome. It only needs to determine where clinical review begins.
Precision Can Hide the Wrong Problem
A system can produce a highly precise queue and still create a dangerous blind spot. If most elevated cases are meaningful, reviewers will learn to trust the signal. That trust is not foolish. No one wants to spend clinical time sorting noise, and a system that consistently surfaces useful cases earns credibility.
Precision inside the queue does not tell you what happened outside it.
We have a receipt for this. The Epic Sepsis Model is a proprietary prediction tool deployed at hundreds of US hospitals. In 2021, researchers at Michigan Medicine ran an external validation across 38,455 hospitalizations and published what they found. The model achieved an area under the curve of 0.63, where 0.50 is a coin flip. It failed to identify 1,709 of the 2,552 patients who developed sepsis, a miss rate of 67 percent. While missing two thirds of the cases it existed to catch, it generated alerts on 6,971 hospitalizations, roughly 18 percent of the hospitalizations examined.
Grant the difference before drawing the lesson. A sepsis prediction model is not a quality review queue. The clinical object is different, and the alert lands on a bedside rather than in a reviewer’s worklist. Resemblance is not identity, and I am not claiming the two systems fail in the same way.
The transferable part is the epistemics. Hundreds of hospitals had deployed that model. Reviewers were working its output daily. The deployed workflow did not expose that miss rate through its own output, because the missed cases generated no alert to inspect. It took a retrospective study, run by people who went looking below the line, to make the blind side visible at all. The study went where the deployed workflow did not. It looked below the line against an independent clinical outcome. That is the control this essay is asking organizations to operationalize.
The organization may know how often reviewers agree with elevated cases, how long each review takes, how often a concern leads to coaching, and how many cases result in escalation. Those are useful operating measures. They do not answer the harder question. What clinically important cases did the system fail to elevate?
Answering that requires looking where the system said not to look. It means sampling below the threshold, reviewing false negatives, comparing performance across clinical contexts, and examining whether some forms of documentation are easier for the system to read than others. It means checking what happens after a model update, a prompt change, a new data source, or a threshold adjustment made to reduce queue volume.
The program can also become best at finding what the organization already knows how to recognize. Clear, well-documented, familiar risks rise. Ambiguous, poorly documented, or unfamiliar concerns remain buried. The queue gets cleaner while the boundary gets less honest.
That work consumes clinical time. It may expose that safe review requires more people than the organization has funded. It may force leaders to choose between a larger queue, slower review, a different workflow, or additional staffing.
If the organization cannot afford to look below the threshold, it cannot claim to know what the threshold hides.
Govern the Boundary
Before trusting an AI-assisted quality review program, I would want to understand the full path from encounter to human attention. What data entered the system? What kinds of clinical meaning were available to it? What caused a case to cross the threshold? What happened to cases just below it? Who could change the model, prompt, rules, or threshold?
More importantly, who owns the blind side?
A clinical quality owner with authority to challenge day-to-day model tuning should own below threshold sampling and false negative review. Independence is the wrong ask, because in most organizations it is unachievable and everyone knows it. Authority is the ask. That work needs a defined cadence and an accountable witness who can verify the results. When misses cross a predefined trigger, leadership must change the threshold, change the workflow, or fund more review capacity.
Owner. Time. Witness. Consequence.
Without those four, “we monitor false negatives” is not a control. It is an aspiration wearing governance language.
Something like this has a shape. A fixed monthly sample of encounters drawn from below the line, sized in advance rather than sized to whatever is left over, stratified so it includes the documentation types the model reads worst rather than the ones it reads best. Reviewed against the same clinical standard applied to flagged cases, by someone whose performance review does not depend on the model looking good. And a miss rate that forces action, set before anyone knows what the number will be.
That last part is the one organizations skip. A threshold chosen after the results are in is not a threshold. It is a negotiation.
Material changes also need receipts. A model update, prompt revision, data source change, or threshold adjustment can alter the effective review population even when the user interface looks identical. The organization should be able to show what changed, who approved it, what population shifted, and how the blind side was tested afterward.
The controls should remain proportional. No one needs to perform a full clinical review on every encounter merely to prove the system might be wrong. That would defeat the purpose and bury reviewers under another layer of safety theater. Some disciplined examination of the unflagged population is still required once the organization begins claiming broader oversight.
The workflow must not translate “the system found no concerning signal” into “no concerning signal was present.” Those statements are not equivalent. Treating them as equivalent turns the absence of an alert into false reassurance.
What the Gate Keeps Out
AI-assisted quality assurance may allow clinical organizations to examine more care than manual review alone. It can surface patterns that would otherwise remain buried and direct scarce expertise toward encounters that deserve a closer look.
Broader coverage does not eliminate the boundary. It makes the boundary more consequential.
When the system determines what reaches the reviewer, it becomes part of the review authority chain. The AI QA signal is not clinical review. It is the gate that decides where clinical review begins. If the organization only measures what passes through that gate, it does not know what the gate kept out.
Somewhere below the threshold is a patient whose worsening symptoms were documented indirectly, whose missed follow-up looked ordinary, or whose treatment pattern did not resemble the risks the model already knew how to recognize. The case never enters the queue. No reviewer opens the chart. No concern is raised. No correction is made.
Later, the absence of intervention looks like evidence that no intervention was needed.
That is not clinical review. It is silence produced by selection.
Human review is only as strong as the signal that reaches the human.
Per ignem, veritas.
Source
Wong A, Otles E, Donnelly JP, et al. External Validation of a Widely Implemented Proprietary Sepsis Prediction Model in Hospitalized Patients. JAMA Internal Medicine. 2021;181(8):1065-1070. doi:10.1001/jamainternmed.2021.2626. Retrieved via PubMed, PMID 34152373.